
Hypercalcemia happens when you have higher-than-normal levels of calcium in your blood. It’s usually caused by primary hyperparathyroidism or certain cancers and is treatable with surgery and/or medication.
What is hypercalcemia?
Hypercalcemia happens when you have higher-than-normal levels of calcium in your blood. Hypercalcemia can be mild or severe and temporary or chronic (lifelong).
Calcium is one of the most important and common minerals in your body. Most of your body’s calcium is stored in your bones, but you need calcium in your blood as well. The calcium in your blood helps:
- Your nerves work.
- Make your muscles squeeze together so you can move.
- Your blood clot if you’re bleeding.
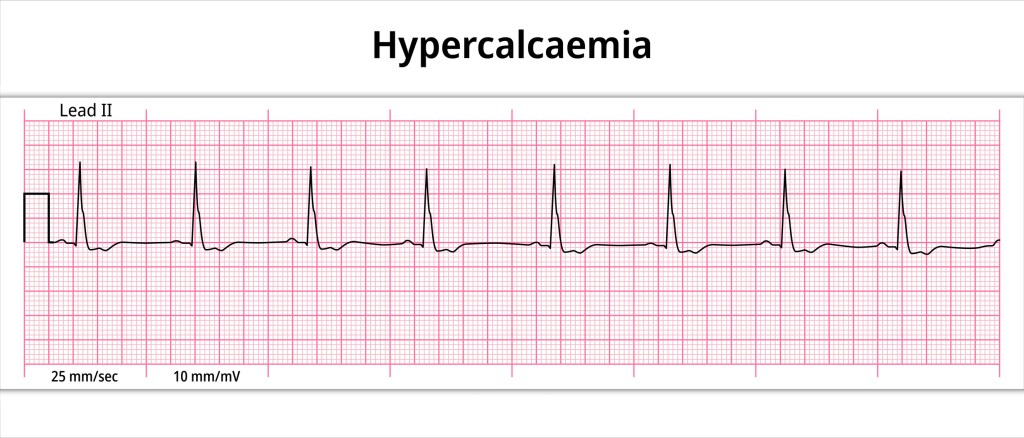
- Your heart work properly.
Two hormones called parathyroid hormone and calcitonin control the levels of calcium in your blood and bones. Vitamin D also plays an important role in maintaining calcium levels because your body needs it to absorb calcium from the food you eat.
Your body normally carefully controls the level of calcium in your blood, but certain medications and conditions can result in high blood calcium levels (hypercalcemia).
What is the difference between hypocalcemia and hypercalcemia?
Hypercalcemia and hypocalcemia are medical conditions that both have to do with the amount of calcium in your blood — the difference is how much.
In the medical world, the prefix “hyper-” means “high” or “too much.” Hypercalcemia means you have higher-than-normal calcium in your blood.
The prefix “hypo-” means “low” or “not enough.” Hypocalcemia means you have lower-than-normal levels of calcium in your blood.
Who does hypercalcemia affect?
Hypercalcemia can affect anyone at any age, but it’s most common in females over age 50 (after menopause). In most cases, this is due to an overactive parathyroid gland.
How common is hypercalcemia?
Hypercalcemia affects approximately 1% to 2% of the general population. Most of the cases — about 90% — are due to primary hyperparathyroidism and cancer-related hypercalcemia (hypercalcemia of malignancy).
Is hypercalcemia life-threatening?
Most cases of hypercalcemia aren’t life-threatening and many people don’t have any symptoms. Healthcare providers often catch it early from routine blood tests.
But severe hypercalcemia can cause more serious problems, including:
- Kidney failure.
- Abnormal heart rhythm (arrhythmia).
- Confusion.
- Coma.
What are the symptoms of hypercalcemia?
Since healthcare provider often discover hypercalcemia in its early stage, most people don’t have symptoms.
More severe and/or long-term cases of hypercalcemia may cause the following symptoms:
- More frequent urination and thirst.
- Fatigue.
- Bone pain.
- Headaches.
- Nausea and vomiting.
- Constipation.
- Decrease in appetite.
- Forgetfulness, depression or irritability.
- Muscle aches, weakness, cramping and/or twitches.
What causes hypercalcemia?
More than 25 separate diseases, several medications and even dehydration can cause hypercalcemia. Primary hyperparathyroidism and various kinds of cancers account for the greatest percentage of all people with hypercalcemia.
Primary hyperparathyroidism and hypercalcemia
In primary hyperparathyroidism, one or more of your four parathyroid glands produce too much parathyroid hormone — the hormone responsible for controlling blood calcium levels.
Your parathyroid glands are located behind your thyroid gland in your neck. Normally, they work with your kidneys, bones and intestines to carefully regulate the level of blood calcium. But sometimes a parathyroid gland becomes overactive, resulting in excess parathyroid hormone release and elevated blood calcium levels.
Cancers that can cause hypercalcemia
About 2% of all cancers are associated with hypercalcemia, and cancer-related hypercalcemia cases (also called hypercalcemia of malignancy) often have a rapid onset and are severe. Certain types of cancer that can cause hypercalcemia include:
- Lung cancer.
- Breast cancer.
- Multiple myeloma (cancer that forms in a type of white blood cell).
- Renal cell carcinoma (a type of kidney cancer).
- Certain cancers of the blood (leukemia).
- Lymphoma (cancer of the lymphatic system).
- Rhabdomyosarcoma (muscle cell cancer).
Medications that can cause hypercalcemia
Common medications and supplements that can cause hypercalcemia include:
- Hydrochlorothiazide and other thiazide diuretics (prescribed for high blood pressure and edema).
- Lithium.
- Excessive intake of vitamin D, vitamin A or calcium supplements.
Taking too much calcium carbonate in the form of Tums® or Rolaids® is actually one of the more common temporary causes of hypercalcemia.
Other causes of hypercalcemia
Other less common causes of hypercalcemia include:
- Lung diseases such as sarcoidosis and tuberculosis.
- Kidney failure.
- Thyrotoxicosis.
- Being bedridden/immobilized for a prolonged time.
- Paget’s disease of the bone.
How is hypercalcemia diagnosed?
Hypercalcemia is a fairly common finding on routine blood tests such as a comprehensive metabolic panel (CMP) or basic metabolic panel (BMP), which include a calcium blood test. These tests allow healthcare providers to detect abnormally high calcium levels early.
The following blood calcium levels indicate different levels of diagnosis and severity of hypercalcemia:
- Mild hypercalcemia: 10.5 to 11.9 milligrams per deciliter (mg/dL).
- Moderate hypercalcemia: 12.0 to 13.9 mg/dL.
- Hypercalcemic crisis (a medical emergency): 14.0 to 16.0 mg/dL.
If you have symptoms of hypercalcemia or are at risk for developing hypercalcemia due to having a certain kind of cancer, your provider will order different blood tests to determine if you have hypercalcemia. If your blood calcium level is elevated, your provider will review your medications and medical history and conduct a physical exam.
If there’s no obvious cause to your elevated levels, your provider may ask you to see an endocrinologist, a provider who specializes in hormone-related conditions, who will provide further evaluation and testing.
What tests will be done to diagnose this condition?
Your healthcare provider may order any of the following tests to help diagnose hypercalcemia and its cause:
- Calcium blood test.
- Parathyroid hormone (PTH) blood test.
- PTH-related protein (PTHrP) blood test.
- Vitamin D blood test.
- Calcium urine test.
If your provider suspects primary hyperparathyroidism is causing hypercalcemia, they’ll likely recommend an imaging test to see if there are any growths on your parathyroid gland(s) or if they’re enlarged. Different imaging tests for this purpose include:
- Ultrasound test.
- Nuclear medicine imaging, specifically a parathyroid scan.
- CT (computed tomography) scan.
How is hypercalcemia treated?
Treatment of hypercalcemia depends on what’s causing it and how severe it is. In mild cases of hypercalcemia, your healthcare provider may tell you to:
- Drink more water.
- Switch to a non-thiazide diuretic or blood pressure medication.
- Stop taking or lower your dose of calcium-rich antacid tablets.
- Stop taking or lower your dose of calcium supplements and calcium-containing supplements, such as multivitamins.
If the hypercalcemia is due to an overactive parathyroid gland, your provider will most likely recommend surgery to have the overactive parathyroid gland(s) removed.
If the hypercalcemia is due to cancer, your provider may suggest any of the following medications:
- Bisphosphonates, such as pamidronate and zoledronic acid.
- Denosumab (XGEVA®), a bone-strengthening medication, for people with cancer-caused hypercalcemia who don’t respond to bisphosphonates.
If the hypercalcemia is severe, and/or causing significant symptoms, your provider may recommend immediate hospitalization for IV fluids and other treatments.
What is the prognosis (outlook) for hypercalcemia?
Prognosis, like treatment, depends on the cause and severity of hypercalcemia. When hypercalcemia happens due to a benign condition or temporary situation, it generally has a good prognosis.
People who have hypercalcemia due to cancer often experience symptoms and require frequent hospitalizations.
What are the complications of hypercalcemia?
Complications of long-term hypercalcemia are rare since calcium levels are checked in routine blood panels and healthcare providers usually catch hypercalcemia early, but complications can include:
- Calcium deposits in your kidney (nephrocalcinosis) that cause poor kidney function.
- Kidney failure.
- Kidney stones.
- High blood pressure (hypertension).
- Depression.
- Bone cysts.
- Bone fractures.
- Osteoporosis.
How can I prevent hypercalcemia?
Not all cases of hypercalcemia can be prevented, but avoiding excess intake of calcium pills and calcium-based antacid tablets can help.
Be sure to talk with your healthcare provider if you have a family history of high calcium, kidney stones or parathyroid conditions. Avoid taking dietary supplements, vitamins or minerals without first discussing them with your provider.
When should I see my healthcare provider about hypercalcemia?
If you have a family history of hypercalcemia and/or hyperparathyroidism, talk to your healthcare provider about your risk for developing hypercalcemia.
If you’re experiencing symptoms of hypercalcemia, contact your healthcare provider.
A note from QBan Health Care Services
Getting a new diagnosis can be stressful. Know that hypercalcemia is treatable and that symptoms usually go away once your calcium levels are back to normal. If you have cancer that can cause hypercalcemia, your provider will likely want to regularly monitor your blood calcium levels. Don’t be afraid to ask your healthcare team questions about hypercalcemia and its management.










